
Pictures courtesy of Dr Tamara Corte, Royal Prince Alfred Hospital 2015
|
Image courtesy of radiopedia.org showing cylindrical bronchiectasis. One can clearly appreciate the tram-track sign which is synonymous for peribronchial thickening.
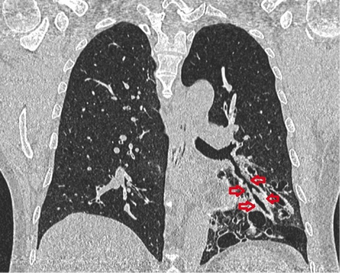
CT findings include increased bronchoarterial ratio, bronchial wall thickening, mucoid impaction, air trapping and mosaic attenuation, signet ring sign |
|

|
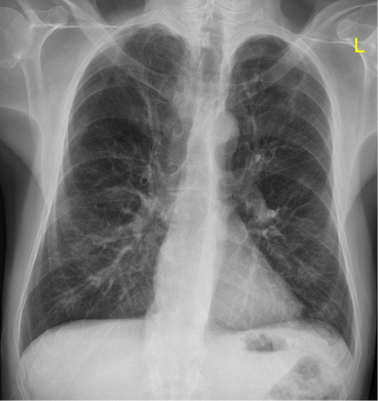
Images above courtesy of radiopedia.org. These two chest X-rays show obvious features of emphysema. Emphysema manifests as lung hyperinflation with flattened hemidiaphragms, a small heart, and possible bullous changes. On the lateral radiograph, a "barrel chest" with widened anterior-posterior diameter may be visualised with a enlarged hyperlucent retrosternal space.
Chest X-ray Comments
- Assess adequacy
- ?Full inspiratory film – want to see 6 anterior rib ends,
- If expiratory film: diaphragms elevated; basal atelectasis; crowding of vascular structures at hilar which can lead to overcalling pulmonary venous congestion; apparent cardiomegaly
- Rotation: clavicles equidistant from the midline
- ?Full inspiratory film – want to see 6 anterior rib ends,
- Note on lateral Xray, lungs should become more hyper-lucent as you move down the lung field
Collapse
- Collapse = volume loss
- Look for secondary signs such as mediastinal shift, elevation of hemidiaphragm, hyper-inflated and hyperlucent remaining lobe
- Consolidation = filling up of air spaces with mucous, pus, water, blood
- Look for maintenance of lung/lobar volume, air bronchograms
- Right upper lobe collapse
- Minor fissures moves upwards
- Collapses upwards and forwards
- Right lower lobe collapse
- Looking for obscuration of the hemi-diaphragm
- Collapse down and towards the mediastinum
- Abnormal diaphragmatic contour
|

|
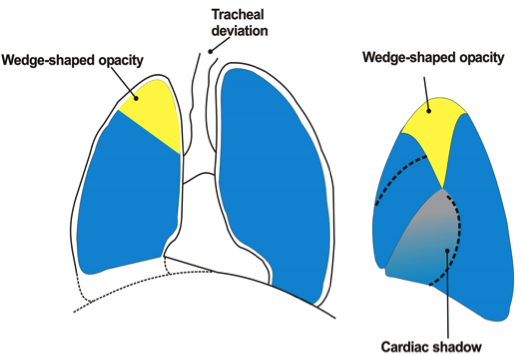
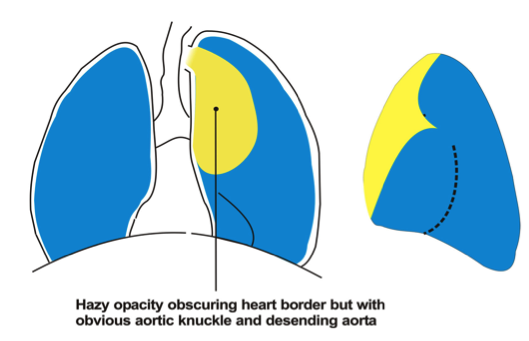
- Left upper lobe collapse
- As no minor fissure, the major fissure moves forward in the chest
- Results in a hazy opacity (aerated lung behind it)
- Abnormal hilum
- Loss of AP window
- Veil like opacity over the left hemithorax – represents collapse upper lobe that has collapsed forward and hyperinflated lower lobe -> implies degree of chronicity
|

|
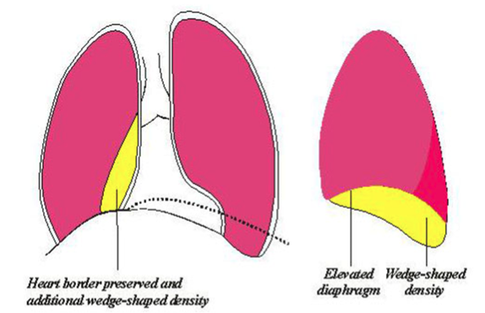
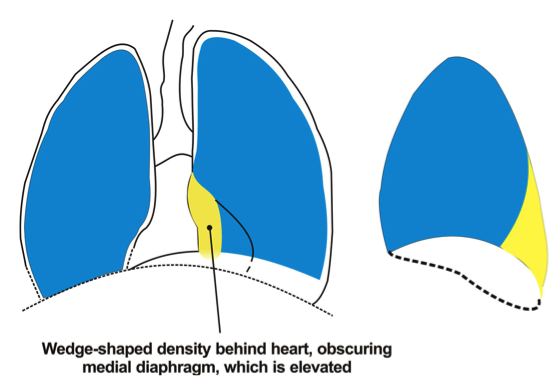
- Left lower lobe collapse
- Looking for obscuration of the hemidiaphragm
- Tracheal deviation to the left
- Diaphragmatic contour can not be differentiated
|
|
