Question 1
What is the most common cause of heart failure with a preserved ejection fraction?
(A) Ischaemic heart disease
(B) Hypertension
(C) Sarcoidosis
(D) Mitral regurgitation
(E) Aortic stenosis
B: PEP lectures 2015. Note that HF-PEF accounts for 30-50% of all heart failure present in the community.
Question 2
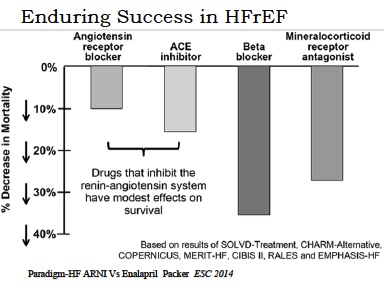
Which of the following has the greatest impact on mortality with regards to chronic therapy of heart failure with reduced ejection fraction?
(A) Beta blockers
(B) Mineralocorticoid receptor antagonists
(C) Angiotensin converting enzyme inhibitors
(D) Angiotensin II receptor blockers
(E) Hydralazine
A: Although they were not head to head trials, beta blockers reduce mortality by ~35%, ACE + ARBS ~ 15%, MRAs ~ 25%. PEP 2015
What is the most common cause of heart failure with a preserved ejection fraction?
(A) Ischaemic heart disease
(B) Hypertension
(C) Sarcoidosis
(D) Mitral regurgitation
(E) Aortic stenosis
B: PEP lectures 2015. Note that HF-PEF accounts for 30-50% of all heart failure present in the community.
Question 2
Which of the following has the greatest impact on mortality with regards to chronic therapy of heart failure with reduced ejection fraction?
(A) Beta blockers
(B) Mineralocorticoid receptor antagonists
(C) Angiotensin converting enzyme inhibitors
(D) Angiotensin II receptor blockers
(E) Hydralazine
A: Although they were not head to head trials, beta blockers reduce mortality by ~35%, ACE + ARBS ~ 15%, MRAs ~ 25%. PEP 2015
Question 3
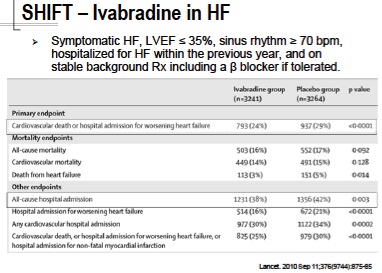
Ivabradine may be prescribed in the setting of heart failure with reduced ejection fractions according to the PBS guidelines. Which of the following is FALSE
(A) Ivabradine blocks hyperpolarisation activated voltage gated Na/K channels on sino-atrial nodal cells
(B) Use of this drug in patients already on background heart failure therapy and with a heart rate of >70 decreases all cause mortality
(C) There is a significant reduction in heart failure mortality
(D) There is a significant reduction in hospital admissions for heart failure
(E) There is NOT a significant reduction in cardiovascular mortality
B : PEP 2015
Ivabradine may be prescribed in the setting of heart failure with reduced ejection fractions according to the PBS guidelines. Which of the following is FALSE
(A) Ivabradine blocks hyperpolarisation activated voltage gated Na/K channels on sino-atrial nodal cells
(B) Use of this drug in patients already on background heart failure therapy and with a heart rate of >70 decreases all cause mortality
(C) There is a significant reduction in heart failure mortality
(D) There is a significant reduction in hospital admissions for heart failure
(E) There is NOT a significant reduction in cardiovascular mortality
B : PEP 2015
Question 4
What is FALSE with regards to BNP
(A) There is NO evidence to suggest that the use of BNP in titrating heart failure treatment reduces all cause mortality
(B) BNP is produced primarily in the atria as a response to myocardial stretch and induces vasodilation
(C) BNP induces naturesis
(D) Endopeptidase inhibitors may increase the levels of BNP and ANP
(E) There is NO grade A evidence for the routine measurement of BNP in guiding heart failure therapy
A: A meta-analysis reported a significant reduction in all-cause mortality for patients with CHF and low ejection fractions that was associated with titrating therapy based on natriuretic peptide levels, but no significant effect on all-cause hospitalisation. Am Heart J 2009; 158: 422-430. Med J Aust 2011; 194 (8): 405-409.
Question 5
What is NOT a risk-factor associated with sudden cardiac death in patients with hypertrophic cardiomyopathy?
(A) Hypertension
(B) sustained VT
(C) Left Ventricular wall thickness >30mm
(D) Unexplained Syncope
(E) Family History of premature sudden death
A: With respect to the ESCARDIO guidelines, if the calculated risk based on history and investigations puts the patient at increased risk of sudden cardiac risk (that is if >6% 5 yr risk) then ICD is recommended.
What is FALSE with regards to BNP
(A) There is NO evidence to suggest that the use of BNP in titrating heart failure treatment reduces all cause mortality
(B) BNP is produced primarily in the atria as a response to myocardial stretch and induces vasodilation
(C) BNP induces naturesis
(D) Endopeptidase inhibitors may increase the levels of BNP and ANP
(E) There is NO grade A evidence for the routine measurement of BNP in guiding heart failure therapy
A: A meta-analysis reported a significant reduction in all-cause mortality for patients with CHF and low ejection fractions that was associated with titrating therapy based on natriuretic peptide levels, but no significant effect on all-cause hospitalisation. Am Heart J 2009; 158: 422-430. Med J Aust 2011; 194 (8): 405-409.
Question 5
What is NOT a risk-factor associated with sudden cardiac death in patients with hypertrophic cardiomyopathy?
(A) Hypertension
(B) sustained VT
(C) Left Ventricular wall thickness >30mm
(D) Unexplained Syncope
(E) Family History of premature sudden death
A: With respect to the ESCARDIO guidelines, if the calculated risk based on history and investigations puts the patient at increased risk of sudden cardiac risk (that is if >6% 5 yr risk) then ICD is recommended.
